Posted: 2026-04-16
🔗 Kavalactones for Agoraphobia: Exploratory Work
This document has been compiled with the gracious assistance of the neuroscientist Kristina Vacy (who has completed their PhD but not had it conferred yet) and who kindly did a partially complete literature review on the liver safety of kava extracts.
Thanks also to John McGowan, lead scientist at Forney Enterprises (Root and Pestle's parent company) for his guidance and generous use of their analytical lab while iterating on the extract.
The concept of using kava for agoraphobia did not originate with them; I came up with it myself and my use was not at their direction.
🔗 Disclaimer
This document discusses the usage of some compounds in the treatment of medical conditions. They have not been approved for the diagnosis or treatment of these conditions. The empirical safety of using them in this way has not been established. Consider this experimental science which should not be replicated outside of an experimental setting.
None of what follows is medical advice; if you have any questions please speak to your primary care physician. Much of what I have done for this project is unwise. Do not attempt it on your own. The following post is effectively pre-science: hypothesis generation for later examination in a more organised way.
🔗 Summary
"The ban on kava in the UK and other countries (e.g. Austria, Germany, France) caused an estimated damage of US$1.2 billion to the industry. Some experts now believe that, all things considered, the ban is no longer justified. But expert opinion is, of course, notoriously unreliable."
~ Expert opinion by Professor Edzard Ernst, M.D. Ph.D.
Published in the British Journal of Clinical Pharmacology
If you say the word "kava" to even an enlightened physician, they will most likely advise you to avoid it, saying that it is a herbal remedy which some people find helpful for mild anxiety, but which is known to damage the liver, especially in high doses.
I've used it extensively for the last 5 years, and this does not in any way tally with my experience and research.
The conclusions that I've come to, along with the science team, are as follows:
We hypothesise that some kavalactones, the active components in kava, in sufficient doses (greater than the accepted ceilings in the literature) may be superior treatments for severe anxiety, as well as a range of other complex conditions, and that, when used correctly, could be unlikely to harm the liver. The circumstances of the liver claims were dubious, and the incentives they were made under are deeply troubling.
Lived experience suggests they may be particularly useful for severe phobic anxiety conditions where benzodiazepines would prevent the formation of emotional memories which are required for recovery.
I'm not claiming there's good academic literature regarding some of the claims I'll be making; on most of these topics academia is silent. This is an n=1 (n=2 in some parts) case study with some interesting implications which are worth exploring, and it fills some gaps with enthusiast and ethnobotanical knowledge.
I have profound and treatment resistant agoraphobia myself, and was fully housebound for some years. My informal research into pharmacology led me to kava, which I found to be a breakthrough: for me, it was significantly more effective than anything I had tried before and also avoided the serious tolerance and dependency issues of many common treatments.
🔗 Hypotheses Worth Examining
We have a large number of interesting claims to examine. If even a fraction of this list holds, it significantly changes the landscape of treatment for severe anxiety conditions. These are the claims this document is implicitly testing:
- Kavalactones are safe at doses well above what Western literature is comfortable with
- Kavalactones can suppress panic attacks if the dose is high enough
- Kavalactones' panic suppression persists for a couple of days
- Kavalactones do not impair emotional memory formation
- Kavalactones do not cause tolerance or withdrawal
- Kavalactones do not trigger or worsen depression
- Kavalactones do not trigger or worsen (hypo)mania
- Kavalactones do not trigger or worsen psychosis
- Kavalactones may enable desensitisation rather than block it
- Kavalactones are safer to the liver than widely believed
- Kavalactones' rare liver harm is caused by glutathione depletion in some cases
- N-acetylcysteine supplementation may mitigate (in whole or in part) rare catastrophic kava-related liver failure
- High potency kava extracts can produce rapid onset via buccal/sublingual administration
- Evidence from the Pacific Islands on kava's safety has been discounted incorrectly
- Agoraphobia is widely misunderstood mechanistically
- Benzodiazepines are mechanistically mismatched to agoraphobia recovery
These all absolutely deserve attention and empirical validation, because they're mostly straightforward to falsify, and if true, then we've already found some extremely high-value information.
As usual, the highest-value part of this is not the answers so much as the questions. There are a lot of interesting questions here, and they are absolutely worth exploring.
🔗 What Is Agoraphobia?
Agoraphobia is commonly defined by laypeople as fear of leaving the house. This is actually the inverse of what it is; a more accurate description would be fear of not being able to get back.
Agoraphobia is usually secondary to uncontrolled panic attacks. The profoundly traumatic nature of severe panic attacks etches sensory or conceptual information into the brain's safety circuitry; whatever circumstances you're in when you panic will become triggers for later panicking. In this sense, agoraphobia is spiritually closer to PTSD than most other anxiety disorders — the principal difference being that the trauma originated in a biological process rather than an external event.
If your worst panic attacks were on rainy or overcast days, you'll feel less at ease on those days even when you're not actively panicking. Same with sunny days, hot days, night time, day time — anything which changes the sensory environment alters your baseline read of safety.
Claustrophobia makes sense to most people. It's a narrow, tight space, and sometimes getting out of it can be hard. If you panic and try to yank yourself you can just get more stuck. Fear of open spaces (kenophobia) actually works more like that than you'd think: you can't actually get out of an open space very quickly — it takes consistent action over time, and locking up from fear will prevent you from doing that.
Kenophobia is not exactly the opposite thing to claustrophobia, but more like an opposite manifestation of a very similar problem. Agoraphobia can present with either, neither or (yikes) both.
In my experience, people consistently try to reduce agoraphobia to psychological "issues" or "fear of responsibility" or things like that — stuff that makes sense to them — because they don't like the idea that this is a deeply biological process which you have no control over.
🔗 Mainstream Agoraphobia Treatments
The usual Official Story is that there are a range of talk-therapy and medication treatments for agoraphobia which have a robust evidence base for effectiveness, therefore, treatable. Patients usually hear this as "curable."
The Official Story is only true in the narrowest and shallowest conceivable sense.
Modern medicine is enough to create some improvement in many cases, but the reality is that these treatments cannot reliably cure this condition except for a very slim (lucky) minority, and that a large chunk of sufferers are simply up shit creek. By any reasonable standard, "treatment resistance" is largely the norm, not an indication that something went wrong.
The happy path for agoraphobia treatment usually looks something like: high dose antidepressants, benzos to cover the gap, cognitive-behavioural therapy to work on reframing and relaxing, and lifestyle changes to reduce stress.
These have giant problems:
- High dose antidepressants are either ineffective or not medically possible for a decent chunk of the population (raises hand)
- Cognitive-behavioural therapy doesn't help everyone and makes some people actively worse (raises hand again)
- Being partly or fully housebound creates stressors of its own, which can create a horrific feedback loop (...yep)
Benzodiazepines, however, are the most problematic of all.
For most people, they quickly and reliably suppress panic attacks and other anxiety, and also feel kind of nice. This is part of the trap: they are highly addictive and withdrawal from even small doses tends to create a mirror-image rebound where the anxiety is greatly increased. I usually describe it as "everything they give you, they take back with interest."
They are also intoxicants, so you shouldn't drive on them, they interact very dangerously with alcohol, and they can result in you making life-changing bad decisions under their influence. Also, in rare cases, they can actually worsen anxiety or behaviour through disinhibition (...raises hand yet again). For these reasons, regulators are becoming increasingly hostile to allowing long-term benzo prescriptions.
But that isn't even the worst part.
Benzodiazepines impair your emotional memory formation. In other words, that lovely relaxed experience you had will not be remembered by your brain's safety circuitry. You actually cannot work on desensitising yourself to the feared stimuli under their influence; it simply doesn't count.
The following work hasn't been clinically validated, but we are hoping that what we have found is a better option.
🔗 What Is Kava?
🔗 Basics
Kava is the common name for a drug made from the root of the plant piper methysticum ("intoxicating pepper"), which is indeed a member of the pepper family.
Much has been written about the various kinds of kava. It's often categorised into wild kava (not safe to consume), tudei kava ("two-day" refers to its prolonged side-effects), and noble kava (suitable for everyday use). Much has been written about this elsewhere.
Because noble kava is sterile, the cultivars are very location-specific; each town has its own varieties, and the effects are sometimes significantly different between them. Kava has deep cultural roots in the Pacific Islands, and each cultivar has a direct connection to the land.
Noble kava grows very slowly, and takes many years before a harvest can be possible; the requirement for a warm climate along with the slow growth makes it largely uneconomical to grow in many other places.
Traditionally, the plant's root is pounded or ground into chips, creating medium grind, the most common form of kava. This is then usually placed in a permeable bag and kneaded with water in a special bowl called a tanoa. The resulting muddy brown liquid is then drunk in one go.
🔗 Legality
In Australia (except for the Northern Territory) kava is legal as a food product. It's a psychoactive food in the same sense that caffeine is. The story of how this came to be is really dumb.
Rural Australia's indigenous/First Nations population has massive problems with alcohol. This is most prominent in the Northern Territory, where the combination of isolation, poverty, lack of opportunities and flaming racism mean that it's one of the leading causes of disability and domestic violence.
Kava was trialled as a safer alternative: the lack of addictive qualities and tendency to cause sleepiness rather than violence made it attractive. Unfortunately, the Murdoch media politicised the drug in an attempt to score points against the Labor administration there, and to this day many people know of kava as "that stuff they gave to the Aboriginals and caused more harm than good", though they can never tell you what the harm actually was other than some emotive vignettes which don't make any sense if you know anything about the drug. Kava was outright banned in the NT, and the ban stands to this day.
In the rest of Australia, kava ended up in a weird legal grey area where it was considered a prescription drug which can't be prescribed, but also was available in very low dose supplements which was better than nothing I guess. There were some efforts to legalise it which never got much interest or traction until they suddenly did.
Basically what happened was that China began attempting to create stronger economic ties in the Pacific Islands. They were proposing to do a kind of Belt and Roads infrastructure upgrade and modernise the region's economy with generous loans. All of a sudden, the Department of Foreign Affairs became extremely interested in the prospect of creating a market for a product which is basically impossible to make anywhere else.
So now we have narrowly legalised kava as a cold water based extraction product; organic solvent extractions are incredibly legally murky. More on that later.
🔗 Pharmacology Basics
Early Western sources saw the drink causing effects that looked like drunkenness to them, and hypothesised that the root was somehow creating an ultra-rapid fermentation of alcohol. Early Western sources on regional cultures are not known for accuracy.
The effects of kava are the result of a range of psychoactive kavalactones. As lactones, they are not water soluble, instead having a high solubility in lipids (fats). Despite this, they are not themselves fats — you can even get them to crystalise.
There are six kavalactones which dominate discussion of kava's effects, each of which differs in subjective character and biological effect. There is no need for me to cover this, because Root and Pestle have already done an outstanding writeup.
The pharmacological interplay between these compounds is astonishingly complex; kava as a whole is an incredibly non-selective drug, with an extraordinary range of mechanisms at play — this is an extremely deep topic and deserves its own discussion.
While numerous kavalactones certainly have activity at GABA sites, it is not the straightforward positive allosteric modulation (PAM) effect you'll get from a benzo (eg. a diazepine PAM — diazepam). It also lacks the less-selective character of alcohol.
The practical upshot of this is: it is very well settled among enthusiasts that kava does not cause tolerance or withdrawals in the sense benzos or alcohol do. There is some controversy over whether the opposite is true — that regular use causes sensitisation instead.
🔗 Subjective Basics
The drink tastes terrible. You know how it looks like mud? It tastes how it looks. It's like an acquired taste, except you never acquire it. It's also not very dense — you might experience effects from a pint worth — and incredibly brutal on the stomach. Vomiting is par for the course.
The kava experience is subtle, and difficult to pin down cleanly. In the traditional form the drug can be, quite frankly, finnicky.
Many people experience nothing the first few times. One friend I shared some with had an instant reaction: "it was like my head just totally emptied and it was all clear and calm." Others have tried many times and still don't understand what it's about.
My experience is: the world becomes softer and smaller, warmer and kinder. The idea of kava as an empathogen is core to my understanding of its effects. It's difficult to put into words exactly, least of all since one of its immediate effects is your internal monologue being greatly turned down in volume.
This is probably very confusing to those who haven't tried it. It's a lot less like alcohol and a lot more like caffeine in the opposite direction.
🔗 Kava for Agoraphobia
Based on my (and one other person's) personal experience, kavalactones seem to have a number of attractive properties when it comes to treating agoraphobia:
- They appear to be highly effective at suppressing or aborting panic attacks;
- They appear to have no tolerance or withdrawal mechanisms; and
- They appear to not impair the formation of emotional memories.
That last one is extremely important for agoraphobia particularly: a fast-acting, non-addictive anxiolytic which is capable of suppressing panic attacks without preventing the formation of emotional memories would be a game changer.
🔗 My Experiences Treating Agoraphobia
🔗 Systematic Desensitisation
Systematic desensitisation is a pillar of cognitive-behavioural therapy (CBT). The basic concept is that you learn relaxation techniques, then create a ladder of increasingly challenging situations and gradually work your way up it. It sounds completely logical if you have not actually lived agoraphobia.
The failure mode that I experienced was going out, doing the thing, and instead of getting a dopamine rush and "yay I can do it!" experiencing "oh my god that was HORRIFYING, I hope I never have to do that again." The cases where a "treatment" becomes endless and pointless torture are high forms of iatrogenic harm. Traditional CBT is what caused my agoraphobia to become profound.
🔗 Dynamics of the Drug
The dosages of kava needed to experience the full antipanic effect are higher than Western literature considers safe. If you have concerns about the safety of dosages of kavalactones greater than 250mg a day, please go to any Pacific Island and tell them that you know better than they do about something they've been doing for thousands of years.
The common formats of the drug unfortunately make it problematic to measure dosage precisely. This is not all bad, though: there are a thousand reasons your anxiety might be higher or lower on a given day, and being able to dose "as you feel" can actually work better than consuming discrete dosage packages.
The most important thing to know about using kava this way: the anxiolytic effect continues for a couple of days. Fascinatingly, I noticed that in those couple of days, I never experienced caffeine withdrawal. I also noticed that my cardio performance was significantly worsened in this timeframe.
🔗 My Protocol
This whole thing would not work if you weren't feeling safe to start with. You need to reach a baseline level of security before you can even think about extending your range.
One of the central problems I'd been having was that I'd walk a certain distance down the street I lived on, then basically lock up and be unable to go forwards or backwards.
The solution I came up with was to use a low-speed E-Scooter and a support worker. If I locked up while scooting, I would simply keep sailing along.
First, he would walk ahead, stop, and then I would scoot up to him. Lather, rinse, repeat.
(Now that I think about it, a natural extension would have been me scooting ahead and him driving to catch up with me after)
Then he got in his car, drove a bit further, and the same.
Then we'd do trips where I drove with him in the car seat.
Then I'd have him drive in front of me and I follow.
Then I'd drive in front with him behind.
And so on.
Success
This is structurally a form of systematic desensitisation. The reasons it worked this time were:
- There was the dynamic social element of working with another person,
- It prioritised rapid movement rather than just standing/walking outside pointlessly suffering,
- Freezing wasn't a problem,
- But above all I had an effective panic suppression drug.
The reality is that kava was the thing which made it able to work this time.
This protocol was unbelievably effective.
Over a matter of months I went from housebound to able to travel around my local area with a support person and even do short trips entirely on my own. I recorded this progress with GPS tracking:
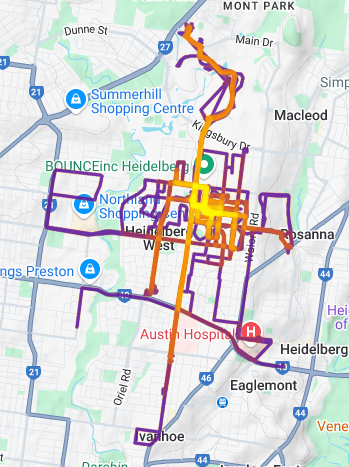
I don't live here anymore. This is just some random person's house now. Please leave them alone.
The other person who used kava for their agoraphobia reported similar improvements.
🔗 Hell
I don't know if I believe in Heaven, but I don't need to believe in Hell, because I've been there. Many times.
Kava's calming effect on me has survived a trial by fire in unthinkable circumstances.
This tanoa has seen some shit:

🔗 Why Kava Is Radioactive
🔗 The Liver Thing
In the 1990s, there was actual meaningful uptake of synthetic kavain under the brand name Neuronika. This drug was approved in several European countries, and the important one was Germany where it was approved for "nervous anxiety, tension and restlessness" — not a diagnostic entity which appears in the DSM or ICD. As a result, clear, evidence-based criteria for how this "condition" would worsen or improve do not exist.
There were a small number of deaths in Europe as a result of the use of Neuronika and some organic solvent kava extracts. I believe the numbers we found are in the order of magnitude of 1 death per million doses.
The German medicine regulator examined kava's approval, and did a cost-benefit analysis on whether it should be continued. They successfully demonstrated that, to everyone's surprise, the drug was not sufficiently effective in the treatment of a condition which does not exist, and in the light of their belief that it was ineffective, concluded that the risk of very rare deaths outweighed no clear benefit.
This is not how the decision was marketed to the public, and to this day it is not how the topic is treated among clinicians and academics. When questioned, the regulator kind of dug their heels in, and that's how we end up with the simplified "kava = liver damage" story that is still so prevalent.
Dr. rer. nat. Mathias Schmidt did excellent presentation slides on this.
As an aside, Germany in the period was one of the world's leading manufacturers of benzos, and the vast majority of deaths weren't actually in Germany, which makes the surrounding incentives feel not one hundred percent pristine.
When you pull in ethnobotanical data, the Western cautions on this substance start to look preposterously ignorant. People in Vanuatu don't have two shells and call it a night: drinking until you can no longer stand is not uncommon.
🔗 Mechanism Speculation
We have a very straightforward theory as to what is actually going on with the liver failure cases. This is a plausible mechanism, not known facts.
Glutathione is one of the primary antioxidants in your liver. It's involved in a range of metabolic processes, effectively "cleaning up" radicals after drugs are broken down.
There is some empirical evidence that many kavalactones deplete glutathione while being metabolised. This is not an exotic toxicity mechanism — it's shared with many familiar drugs like paracetamol. Water-based extractions of noble cultivars are empirically known to contain (water-soluble) glutathione as a component.
This would neatly explain the delightful "Pacific paradox" of why Islanders do not experience liver injury: the traditional preparation of kava involves creating an emulsion of water-insoluble lactones in a slurry which contains glutathione. In this theory, their livers are protected because the root contains the very chemical being depleted, and the traditional production process retains it.
It also creates a falsifiable prediction: that organic solvent kava extracts may be able to solve the rare liver problems by incorporating a bioavailable source of glutathione (eg n-acetylcysteine).
With that being said, Schmidt has cast doubts on this theory, so it's not settled.
As an aside on the "Pacific paradox", many studies threw out data points from the Pacific Islands due to lack of medical infrastructure, like it's Lord of the Flies over there and nobody would notice people dropping dead en masse.
🔗 Extraction
We've come up with a straightforward process to create a high-potency extract which can be used portably and discreetly in public — the use case is similar to "a bar of Xanax in your bag you touch twice a year" — an "off-switch" for panic attacks which you keep so you don't need it (ie you can endure more when you know you have the option). With careful cultivar choice, you can tweak the effect profile. We have validated the chemistry of the product in an analytical lab which generously donated their time.
Similar products are available overseas, but not in Australia.
I'm going to be strategically silent here so as not to encourage people to experiment.
Also, the major progress I made with the help of kava was not using the extraction; that happened later.
🔗 Barriers to Adoption
We investigated what it would take for something like this to ultimately become a medication that a doctor would prescribe. I did not think it was possible for me to become any more cynical about medicine and pharmaceutical development, but here we are.
The TLDR: the incentive structure strongly points against kavalactones being turned into a medicine. It is possible to patent an existing compound for a new use (this is regularly stretched to its limit, a la esketamine), and there are no dedicated medications for agoraphobia proper, but everything else points against it for purely regulatory/financial reasons.
Whole kava and cold water extractions are legal as foods. Organic solvent extracts can only be marketed as schedule 4 (prescription only) medications. That doesn't make them illegal to possess or consume, but actually marketing them requires an approved indication with clinical trials etc. This process is fabulously expensive and risky to go through, and it would likely be near-impossible to get buy-in for that investment.
The most likely scenario I can imagine is a drug development firm making a slight tweak to a molecule and presenting it to regulators as a fresh new (likely inferior) product. If this is how it can become a thing, that's fine, but the drug development process is actively pushing us away from an easy pre-existing answer.
🔗 Observed Side Effects
Excessive Jolliness
A most peculiar side effect. Given the nature of the conditions that this might be useful for, this is probably not a bad thing.
Reduced Cardio Performance
This continues for the entire (couple of days) period of panic suppression.
Somnolence
The effect of kavalactones on sleep is mixed and complex. They can absolutely cause sleepiness, but they can also absolutely keep you awake. Chemotypes matter here, as well as the mechanics of dosing.
Sound Intolerance
A desire for quiet, or at least not intrusive sounds.
Demotivation
Kava reduces productivity.
Restlessness
Paradoxical but real.
Muscle Relaxation
This seems to be dihydrokavain mediated and can look like drunkenness from the outside.
Temperature Perceptual Weirdness
Kava can cause you to feel hot and cold at the same time.
Double Vision
This seems to be dihydrokavain mediated and connected to muscle relaxation.
Retching/Vomiting
Most of this is the result of the volume and miscellaneous plant matter in the traditional drink, but not all of it.
Even the mostly-kavain extract still had some of this effect, albeit many hours later, suggesting that high doses of kavain are directly one of its mechanisms. Acidic drinks seem to help a little.
Digestive Problems
Similar to the retching, just downstream.
Compulsive Re-Dosing
Not so much like an alcohol addiction, more like potato chips: "once you pop you can't stop".
Does not seem to be kavain mediated — cultivars which are heavily kavain-dominated don't seem to have this effect.
Dry/Flaky Skin
This is often thought to be the result of something in particulate matter from the traditional drink. An extract may not have this problem.
Impaired Judgement
Kava can cause alcohol-style impaired judgement, but only at extremely high doses. By my estimation, you would have to reach the point where it's difficult to stand before this becomes a problem.
Checkin
Written on: 7.5mg olanzapine since 2025-11-11, varying dose since 2006
Cognitive capacity: poor - estimate 25% brain